(See related pages)
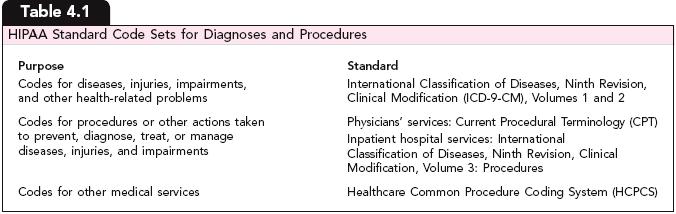
As a part of the medical billing process, medical coders in the health information management (HIM) department assign codes to patients' conditions and procedures. These codes are reported on claims to represent the services the facility provided for the patient and the medical necessity of those services. Clearly connecting what was done—the procedure code—with why it was done—the diagnosis code—is essential for maximum appropriate reimbursement. For this reason, patient account specialists need to understand the basics of the medical coding process. As explained in Chapter 1, HIPAA mandates certain medical code sets—standardized alphabetic and/or numeric representations of data—for use in health care transactions. Table 4.1 summarizes the three classifications.
Learning ObjectivesDiscuss the purpose of ICD-9-CM.Describe the organization and content of Volumes 1, 2, and 3 of ICD-9-CM. Understand the conventions that are followed in ICD-9-CM. Identify the purpose and correct use of the present on admission (POA) indicator. Discuss the purpose of the procedural codes in the HCPCS/CPT code sets. Describe the structure and content of the index and the main text in CPT. Describe the purpose and correct use of CPT modifiers. Describe the structure and content of HCPCS. Describe the four-step process medical coders follow to assign correct ICD-9-CM and HCPCS/CPT codes. Identify the code sets that are associated with inpatient and outpatient billing for hospital services. |